Proper diagnosis is key in properly managing a chronic cough. The first step is ruling out a source in the lungs or bronchial airways. Certain heart problems may also cause a cough and this must also be ruled out.
This is a typical profile for a patient presenting with a chronic cough in this office:
This is a typical profile for a patient presenting with a chronic cough in this office:
- All previous diagnostic examinations are normal.
- Typical cough medicines (except those with Codeine), are ineffective.
- Dry cough (no significant mucous is coughed).
- Cough began during or after an upper respiratory illness (i.e., could, flu).
- Cough has been persistent for several weeks, months or even years.
- Coughing now is commonly triggered by a tickle.
- Patients wake up coughing.
- Coughing can lead to sense of being strangled, even vomiting.
The Diagnosis: Irritable Larynx Syndrome (ILS)
(previously also known as Hypersensitive Larynx Syndrome, HLS)
In many cases, patients experiencing a chronic cough with no known cause are diagnosed by this practice as experiencing irritable larynx syndrome. This is something the SLP staff is very effective in treating, provided there is adequate patient compliance with prescribed protocols.
Before this diagnosis can be made, an otolaryngology examination will be conducted to examine both the structures as well as function of the throat. The examination typically includes one or both of the following endoscopic examinations that allow for close examination of the larynx and vocal cords (where a cough is typically triggered).
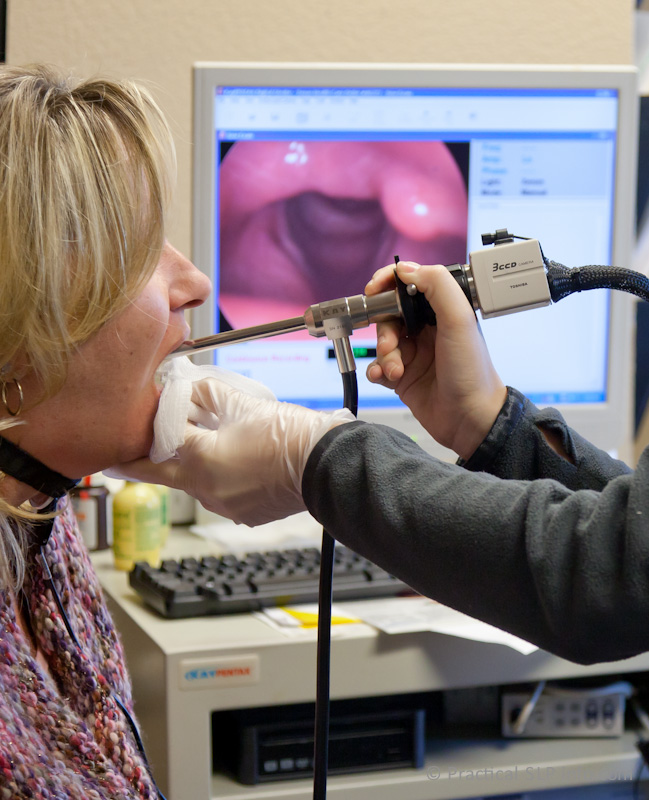
Flexible Fiberoptic Endoscopy For this examination, a nasopharyngoscope is passed through the passageway of the nose into the throat. The endoscope allows for visualization of the structures of the throat, in this way, assessing the overall health and status of the various structures. In some cases, you may be referred for closer assessment of the larynx (voice box) using Stroboscopy.

Stroboscopic Examination
Stroboscopy is an endoscopic procedure that utilizes advanced technology to closely examine the larynx. During this examination procedure a rigid endoscope is utilized in combination with strobe lighting. This allows for magnified imaging of the larynx and surrounding structures as well as for direct visualization of the vocal cords during vibration.
**Many times, clinical changes indicating worsening, stability or improvement in the condition of the laryngeal structures are best assessed with stroboscopic examination. For this reason, following your initial diagnosis, you may be monitored with periodic stroboscopy.
Endoscopic - Stroboscopic Findings
There can be significant inflammation of the vocal cords, due in large part to the persistent and traumatic coughing behavior. There may be inflammation of other portions of the larynx as well, most commonly, the back (posterior sections), when laryngopharyngeal reflux is a component to the hypersensitivity. There are otherwise normal exam findings.
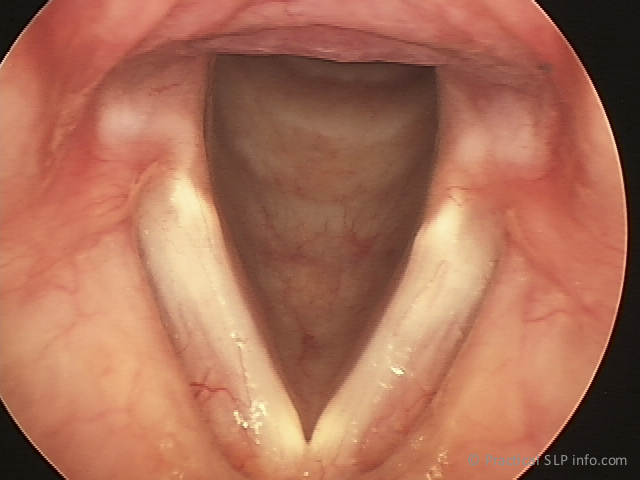
Healthy Larynx
|
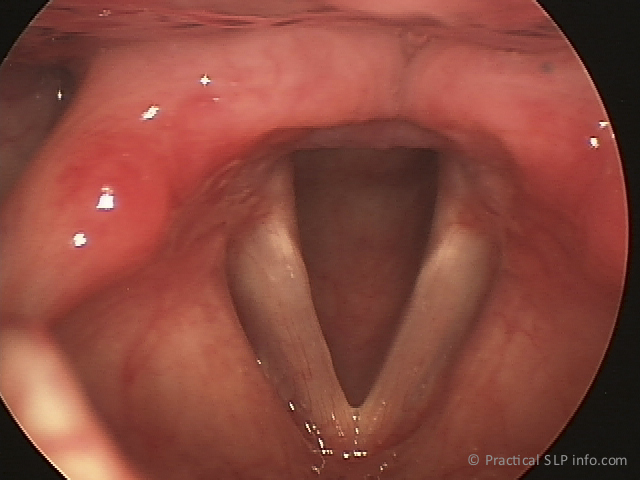
Irritable Larynx
|
